The renaming of PCOS to PMOS is the most consequential disease-nomenclature overhaul in a generation
For decades, clinicians and patients have operated under a name that was quietly doing damage. Polycystic ovary syndrome (PCOS) implied the problem was cysts on the ovaries. But many patients never develop ovarian cysts. Meanwhile, the broader metabolic and endocrine devastation that was taking place (insulin resistance, cardiometabolic risk, androgen excess, irregular cycles, infertility, mental health consequences) went systematically underrecognized, underdiagnosed, and undertreated.
On May 12, 2026, that name was formally retired. A global consortium of 56 leading academic, clinical, and patient organizations voted 88 out of 90 to adopt the new designation: Polyendocrine Metabolic Ovarian Syndrome (PMOS).
What PMOS Actually Looks Like in Your Patients
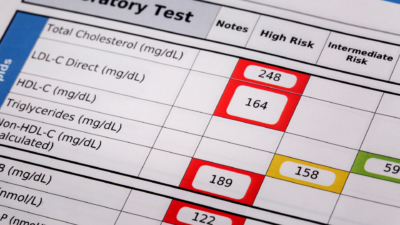
PMOS is a multisystem endocrine disorder. Some patients present with classic androgen excess and cycle irregularity while others lead with metabolic features like weight gain, glucose dysregulation, dyslipidemia with no cysts in sight. The old name created a funnel that most patients didn’t fit through.
For pharmacists managing these patients, the therapeutic landscape includes multiple drug classes: insulin sensitizers (metformin remains first-line for metabolic features), oral contraceptives (for androgen suppression and cycle regulation), ovulation inducers (letrozole, clomiphene), and increasingly, GLP-1 receptor agonists for the cardiometabolic overlap. Anti-androgens (spironolactone, finasteride) come into play for hirsutism and alopecia. None of these are simple, and polypharmacy risk is a real concern.
A Three-Year Awareness Ramp Is a Revenue Window
PMOS affects roughly 13% of reproductive-age women, with 70% undiagnosed. That population is already at the pharmacy picking up metformin, spironolactone, or an OCP without a unified diagnosis connecting them. The rename, paired with updated clinical guidelines expected over the next 12–18 months, opens the door for structured PMOS pharmacist services: collaborative practice agreements, point-of-care A1c and lipid screening, and MTM sessions built around the PMOS metabolic phenotype.
Pharmacies that move first on education, service packaging, and provider communication become the community anchor point for PMOS care coordination.
Three Moves to Make While the Window is Still open
1. Update MTM intake language. A patient on metformin for “blood sugar” plus spironolactone for “acne” plus an OCP may never have been told these are mechanistically connected. You can make that connection and document it.
2. Create a patient handout. A clear, one-page explanation of the name change and what PMOS means, with questions to bring to their provider, is a high-value touchpoint patients remember.
3. Send a prescriber update. A brief, clinical note to local endocrinology, OB/GYN, and primary care practices positions your pharmacy as current. Low cost. High credibility.
The Male Analog Question And Why the Consortium Didn’t Wait
One contested element: whether to drop “ovarian” entirely to accommodate a potential male expression of the syndrome. Early research suggests men with elevated androgens, insulin resistance, and specific metabolic profiles may share underlying pathophysiology. The consortium decided the evidence wasn’t ready and that expanding the name prematurely risked diluting resources and shifting clinical attention away from a population already underserved by research funding.
Further renaming would require dramatic changes in the science. For pharmacists, PMOS is stable, but the metabolic and endocrine lens it introduces is likely to expand as research catches up. Watch for new guidelines from the Androgen Excess Society, evolving GLP-1 indication data in PMOS, and updated CPIC guidance for agents commonly used in this population.
Sources & Further Reading
World Health Organization — PCOS/PMOS fact sheet
Teede HJ et al. — The Lancet, May 12, 2026 — The original global consensus paper
Lebanova H et al. — Pharmacy, 2025 — Pharmacist role in PCOS drug-related problems
Merelli A. — STAT News, May 12, 2026 — The story behind the rename
University of Colorado Anschutz — May 12, 2026 — Expert commentary on the name change