The most common chronic liver disease in the world doesn’t get much time in pharmacy continuing education. It doesn’t dominate clinical pharmacy conferences. It doesn’t trend on health news feeds. But 1.3 billion people have it, it sits directly in the patient population you already manage, and Pharmacy Times this week named it one of the most urgent underaddressed opportunities in frontline pharmacy practice.
Meet MASLD, and start thinking about which patients in your panel already have it.
What MASLD Is and How the Name Changed
Metabolic dysfunction-associated steatotic liver disease, MASLD, is the leading cause of liver disease globally, affecting up to 30% of the global population at varying degrees of severity. The name changed from non-alcoholic fatty liver disease (NAFLD) in 2023 following international consensus. The goal was to reduce stigma and replace exclusionary descriptors with terminology that names the actual mechanism: metabolic dysfunction.
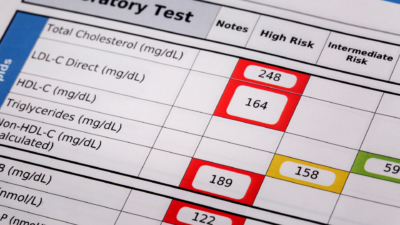
The rename matters clinically. MASLD is defined by the presence of hepatic steatosis, fat accumulation in liver cells, alongside at least one cardiometabolic risk factor: overweight, hyperglycemia, hypertension, or dyslipidemia. Alcohol use is not a prerequisite for exclusion. Metabolic disease is the driver.
In 2021, researchers counted 1,267.9 million MASLD cases globally. The age-standardized prevalence increased 24.3% since 1990. High fasting plasma glucose is the leading modifiable risk factor.
Projections place MASLD cases in the United States at 100.9 million by 2030, up from 83.1 million in 2015. MASLD is simultaneously one of the fastest-growing areas of liver research and one of the most overlooked conditions in the national obesity epidemic.
Why This Is a Metabolic Disease Problem Not a Liver Specialist Problem
The instinct is to think of MASLD as a gastroenterology or hepatology issue. That instinct is wrong, and it’s why 1.3 billion patients remain underidentified.
Most individuals with MASLD, and most of their healthcare professionals, remain unaware of the severe hepatic and extrahepatic health risks associated with the condition and the need for early identification. The American Diabetes Association issued a consensus report in June 2025 describing this as a call to action: screen for liver fibrosis and risk stratify people with prediabetes or type 2 diabetes, if obesity is also present. Liver steatosis affects approximately two out of three people with type 2 diabetes.
Two out of three people with type 2 diabetes. That is your patient panel. Every patient you manage for metformin refills, GLP-1 adherence, blood pressure, or high triglycerides is potentially a patient who has undiagnosed MASLD, and no one has told them.
MASLD can progress from benign hepatic steatosis to metabolic dysfunction-associated steatohepatitis (MASH) when inflammation develops. From there, about 6–7% of individuals with simple steatosis develop early fibrosis each year, and 5–9% progress to more advanced fibrosis stages annually without intervention. Approximately 20% of MASLD patients progress to MASH, and 15–20% of those with MASH can develop cirrhosis over 15–20 years.
The disease progresses silently. Patients feel nothing until significant damage has already occurred. Early detection, at the steatosis stage, before inflammation and fibrosis, is where intervention works.
The Weight Loss Data That Reframes Everything
The most powerful treatment for MASLD right now is not a drug. It is weight loss, and pharmacists already deliver weight management support every day.
Lifestyle intervention remains the cornerstone of MASLD management. Sustained weight loss of 5% or more reduces hepatic steatosis. Weight loss of 7% or more improves necroinflammation. Weight loss of 10% or more stabilizes or reverses fibrosis.
Among patients who achieved 7% total body weight loss, 64% had MASH resolution. In patients who lost 10% of their total body weight, 45% had fibrosis regression by at least one stage, and the remaining 55% had fibrosis stabilization. In patients with higher weight loss of 10% or more, 90% had resolution of steatohepatitis.
Those numbers describe what a GLP-1 therapy already delivers for millions of your patients. Semaglutide and tirzepatide, GLP-1 receptor agonists, produce mean weight losses of 15–22% in clinical trials. Mediterranean diet patterns rich in lean proteins improve insulin sensitivity and liver outcomes.
Every patient on a GLP-1 for diabetes or obesity may be simultaneously treating undiagnosed MASLD. Whether they benefit depends partly on whether anyone monitors that connection and explains it to them.
The Drug Pipeline Every Pharmacist Must Know
Until recently, no FDA-approved pharmacological therapy existed specifically for MASLD. That changed in 2024.
Resmetirom is the only current FDA-approved pharmacologic therapy for patients with F2-F3 fibrosis, the intermediate and advanced fibrosis stages where liver damage has already progressed significantly. Several additional emerging therapies sit in the research pipeline.
The most extensively studied investigational drug classes include GLP-1 receptor agonists, PPAR agonists, and FXR agonists, as well as inhibitors of ACC and DGAT. These therapies show promising effects on hepatic steatosis, liver enzyme levels, and metabolic markers and may reach clinical practice soon.
This means the MASLD pharmacotherapy landscape will expand significantly within the next three to five years. Pharmacists who understand the disease mechanism, the fibrosis staging system, and the drug classes under investigation now will be the ones their prescribers and patients turn to when new agents reach approval.
The FIB-4 Score: 30 Seconds, Existing Labs, Clinical Transformation
You don’t need a liver biopsy, a specialist referral, or an imaging appointment to identify which of your patients may have advanced liver disease. You need four values that many of your patients already have in their labs: age, AST, ALT, and platelet count.
FIB-4 is a simple, non-invasive index for liver fibrosis risk stratification calculated from age, AST, ALT, and platelet count. The formula is: (Age × AST) ÷ (Platelets × √ALT). It is widely used as a first-line triage tool for identifying patients who may have advanced hepatic fibrosis. It is endorsed as Step 1 in the NICE and EASL fibrosis assessment pathways.
The most used cut-off values for assessing advanced fibrosis in MASLD are 1.30 and 2.67. A FIB-4 score below 1.30 indicates low risk, scores between 1.30 and 2.67 are indeterminate, and scores above 2.67 suggest high risk for advanced fibrosis.
MASLD is often asymptomatic until advanced fibrosis develops. Early detection is key to preventing both liver-related and cardiovascular complications. FIB-4 enables risk stratification in primary care settings without the cost, invasiveness, or risk of a liver biopsy.
For patients aged 65 and older, the threshold shifts slightly: use a low-risk cutoff of 2.0 rather than 1.3, because age inflates the score in older populations. For patients under 35, sensitivity decreases, and clinical judgment becomes more important.
The workflow is simple. Pull up a recent comprehensive metabolic panel. Enter age, AST, ALT, and platelets into a free FIB-4 calculator, multiple apps and websites provide one in seconds. Interpret the score. If the result lands in the indeterminate or high-risk range, document it and recommend hepatology referral through the patient’s primary care provider.
That single action, run the FIB-4, report the result, recommend follow-up, positions you as a pharmacist who caught something that matters. Primary care physicians often don’t calculate FIB-4 in routine diabetes visits. You can.
The Pharmacist’s Expanding Role
Management of MASLD in adults involves an interprofessional team, primary care physicians, endocrinologists, nurses, registered dietitians, behavioral health specialists, obesity management teams, pharmacists, and liver specialists. The comprehensive care plan includes lifestyle modification, weight management, and pharmacological treatment aimed at preventing cardiovascular disease and MASH cirrhosis.
The projected scarcity of specialized healthcare professionals, particularly hepatologists and gastroenterologists, makes pharmacists’ role pivotal in NAFLD/MASLD management. Timely identification and community-level intervention can prevent progression to chronic liver disease.
Community pharmacists sit at exactly the right point in the care continuum: frequent patient contact, longitudinal medication relationships, and direct access to the metabolic patient population most at risk. The pharmacist who screens for MASLD, calculates FIB-4, counsels on GLP-1 therapy as a liver benefit (not just a diabetes or obesity benefit), and coordinates referrals for high-risk patients delivers a clinical service that most patients have never received from anyone.
Your Action This Week
Start by changing how you look at three patient categories you already manage:
Type 2 diabetes patients. Two out of three have MASLD. Most don’t know it. Pull their most recent CMP. Calculate FIB-4. Flag any indeterminate or high-risk scores for prescriber communication.
Obesity patients on GLP-1 therapy. They may already be treating undiagnosed MASLD. Explain that connection explicitly. Add liver enzyme monitoring to your counseling protocol for new GLP-1 starts.
High triglycerides, hypertension, or metabolic syndrome patients. Each of these is a cardiometabolic risk factor that, by definition, elevates MASLD risk. Ask directly: “Have you ever been evaluated for fatty liver disease?”
The 30-second FIB-4 calculation doesn’t require new equipment, a new workflow system, or a new clinical service model. It requires the labs that already exist in your patient’s record and the clinical knowledge to interpret them.
1.3 billion people have this disease. Most don’t know it. You are the most accessible healthcare professional in their lives. Start asking.
Sources: Pharmacy Times (MASLD: Expanding Pharmacist Role in Frontline Practice, 2026), PMC (Pharmacological Treatment of MASLD: Contemporary Treatment and Future Perspectives, IJMS 2025), PMC / MDPI (Diet and Lifestyle Interventions in MASLD: A Comprehensive Review, 2025), PMC (Emerging Perspectives in the Diagnosis and Management of MASLD: A Narrative Review), PMC (Global Burden of MASLD: Trends 1990–2021 and Predictions to 2030), American Diabetes Association / Diabetes Care (MASLD in People With Diabetes: A Consensus Report, June 2025), AASLD (Steatotic Liver Disease: Cutting Through the Fat; Noninvasive Assessment of MASLD), PMC (Expanding Pharmacists’ Role in NAFLD Management, 2023), PMC (FIB-4 as a Screening and Disease Monitoring Method in Pre-Fibrotic MASLD), PMC (Identifying and Linking Patients at Risk for MASLD with Advanced Fibrosis in Primary Care), European Medical Journal (FIB-4 Score Reliability in Liver Screening, March 2026), AASLD Liver Fellow Network (FIB-4 Score Interpretation and Cut-offs), PMC (Weight Loss in MASLD Restores Balance of Liver Fatty Acid Sources)